TAVI - CoreValve (Medtronic)
Transcatheter Aortic Valve Repair (Wikipedia) procedures utilize a femoral approach to deliver a stent-based aortic valve to the patients heart. There are two valve types available:
This procedure is usually done in Room 1, and requires a 5 person team: Front table scrub, Back table scrub (device prep), Circulator, Pacer/Circulator, and Recorder. The rep for the respective company will be present to assist with device prep except in the case of an emergency valve placement.
In rare cases, the BASILICA procedure will be necessary to split the existing valve leaflets to prevent blockage of the coronary arteries. In that situation, the equipment on the BASILICA page will be needed in addition to the equipment listed below.
Per Rosalie:
TAVR/TMVI
- Edwards Sapien 3 Ultra (20, 23 & 26mm) and Sapien 3 (29mm) – scan the valve barcode (box) in Epic for documentation and charges. Bundle includes valve, delivery system, crimper, e sheath intro set, balloon cath & locking syringe.
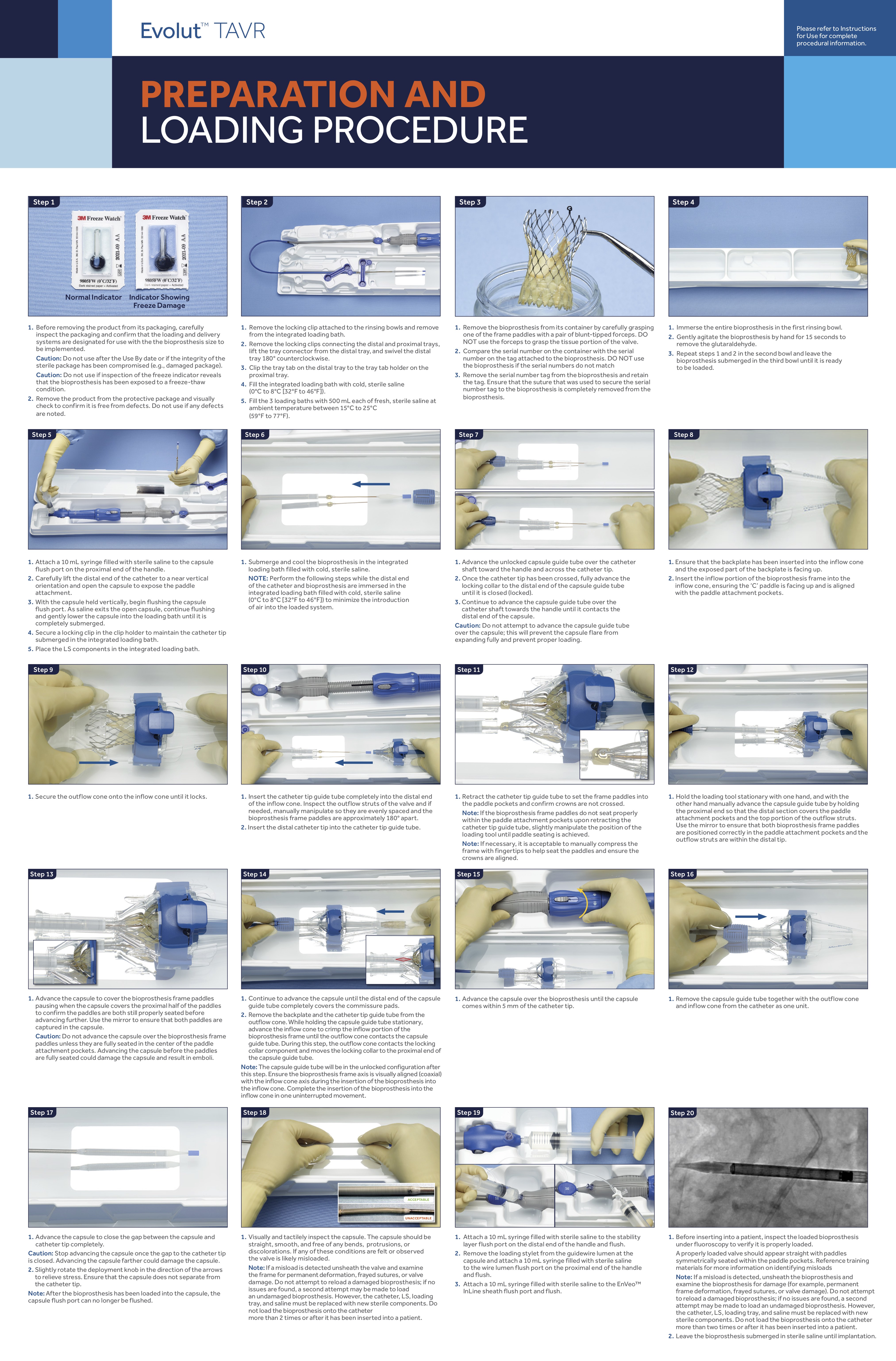
- Medtronic Core Valve – all items are charge separately. Scan all barcodes (delivery system, loading system and valve).
Daniels/Spies - Draft
ACIST A1000V SYRINGE USED WITH 50/50 CONTRAST MIX
**If the patient has an existing RBBB, prep the right chest and no rampart.***
Sheaths:
- 5Fr Micropunture Kit
- FOR DANIELS - 6Fr Slender ( Not needed for valve-in-valve)
- FOR SPIES - 6F x 10cm sheath
- 8Fr x 10 cm sheath
- SHEATHLESS INLINE DELIVERY: 18F coons dilator and 14F Cook sheath post. (Do not open until confirmed during timeout)
- 18fr Dryseal if sheath delivery system is used or when doing a BAV.
Wires
- (2) Cordis 150J
- Cordis 260J
- Safari
- Terumo Stiff Straight Glidewire 0.035 x 150 cm
- 1.5mm J Glidewire (not needed for spies)
- Amplatz 7cm tip IF USING dryseal
- .035 Standard Straight for Valve-in-Valve crossing, no need for glidewire.
Catheters:
- 5Fr AL1 diagnostic (5F JR4 diagnostic to cross valve for Spies)
- 5Fr Ang Pigtail
- 5Fr Str Pigtail
- 5Fr Tig (when doing coronary angiography) OR 6F JL4/JR4 for spies
- Valve-in-Valve cases: Mosaic valve needs pigtail, all others do not
Medications on table:
- Lido/Bupivicaine 50/50
- Epinephrine 10mcg/ml in red medallion syringe (From anesthesia)
- BACK TABLE ; 2 L of cold saline for delivery catheter prep ; 1 L room temp Hep saline for front table ; 1 L room temp saline for back table
Miscellaneous Supplies
- Acist hand control
- Solopace Remote
- 2L cold saline
- (3) Perclose
- Spies 22G Grey Lido Needle
- Dual Red/Black Pacing Remington cables
- EP Quad Cable
Unipolar Transvenous pacing supplies.
- Alligator Clip Remington Pacing Cables
- TZ Medical Defibrillation Pads - Found in EP pyxis in labs. Large pad utilized as a grounding pad on the patients chest (subxyphoid)
- NOTE : If patient is in second degree HB please prep RIJ
Procedure
- Contralateral arterial access - 6fr. Sheath (normally LFA) using micropuncture. Verify wire position with fluoro and save an image.
- Primary access - with micropuncture. Verify wire position with fluoro and save an image
- Pre-close x 1, sutures secured with hemostat.
- 8F sheath reconstituted and advanced after pre-closure.
- Straight Pigtail -> LFA -> AO root injection
- Standard Injector settings (adjusted based on pt and root size)
5/5 on Acist
- AL1 advanced through 8F sheath over standard J.
- Standard J removed and crossing wire advanced. Cross valve. Wire removed.
- Measure EDP and gradient...maybe
- Working wire advanced to LV. AL1 removed.
- 8F sheath removed and 18 F dilator in and out OR 16 F dryseal advanced depending if doing in-line or not.
- Check valve under fluoro for markers
- Insert valve delivery system
- Multiple AO grams for positioning
- Test pacing on Safarii wire
- Rapid pace 160, check for capture, 220 burst
- Pace -> AO gram -> Slowly deploy valve
- Cine length set at 40 seconds or more
- TTE
- Pigtail advanced to remove working wire from LV
- Pigtail readvanced to AO for AO gram (15/30 standard injection)
- Delivery system removed and 14F sheath advanced.
- Have second perclose, tools and dilator ready
- Protamine given, Preclosures completed, manual pressure for 5ish minutes
- Pigtail pulled back to iliac bifurcation and subtracted iliac angio performed (6/18 on Acist)
- Pigtail removed
- Secondary access Perclosed
- Dermabond all access sites, no dressing needed.